Non-Surgical Minimally Invasive Technique for the Treatment of Primary (Hepatocellular Carcinoma) and Metastatic Tumour.
Transcatheter Arterial Chemoembolization (TACE) and Radiofrequency Ablation (RFA)
PRECISION TACE
Recently, minimally invasive interventional radio-logical therapies are found to be effective in both primary tumors & metastatic tumors. These therapies may replace surgical resection in the near future.
Chemoembolization for liver tumor
Most patients with HCC are diagnosed at intermediate to advanced stage, and there is no standard treatment for these patients. Definitive surgical intervention is not feasible in most cases due to extreme tumor extension, multiplicity of tumor foci & associated liver cirrhosis at the time of diagnosis.
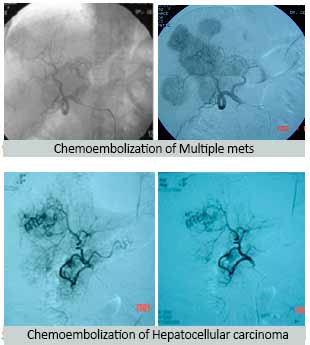
Only 10-20% of patients of HCCs are eligible for resection & even after curative resection, post-operative recurrence is common. Because of these reasons, transarterial chemoembolization has been aggressively tried to treat HCCs by Interventional Radiologist and it improves survival of patients with unresectable HCC and is likely to become the standard treatment.
We are 1st in the country to treat a patient of unresectable Hepatocellular Carcinoma by PRECISION TACE (transarterial chemoembolization) with newly introduced Drug Eluting beads (DC Beads).
This drug eluting bead is specifically designed to be loaded with cancer medicine (chemotherapy drug), This Drug Delivery Embolization System brings a new level of efficacy accuracy and convenience to trans-arterial chemo-embolization. In addition there are other advantages like it requires lower dose of cancer medicine in the system and allows higher doses of cancer medicine in the tumor for longer time, and it is a consistent treatment.
Chemoembolization is a dual therapeutic approach involving Concomitant hepatic artery embolization and Infusion of a concentrated dose of chemotherapeutic drugs.
Procedure: –
It is a minimally invasive Interventional Radiological procedure, which means it requires only a tiny nick in the skin. It is performed under sedation and local anesthesia – feeling no pain and usually requires a short hospital stay.
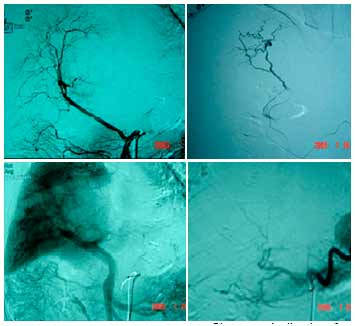
The Interventional Radiologist makes a small nick in the skin at groin, insert a catheter, identifies arteries supplying to tumor(s) by using angiography with contrast media injection and then inject drug eluting bead loaded with chemotherapy drug (cancer medicine) that block the tiny vessels supplying the tumor (s). This blockade of blood supply to the tumor causes infarction and delivering a high concentration of drug to the target tumor (s) for longer time while reducing systemic toxicity.
Ideal Patient for PRECISION TACE
(Trans-arterial chemoembolization) should meet following basic requirements:
- Patient with diagnosis of unresectable hepatocellular carcinoma.
- Patients with tumour size of 5 cm or more. (Tumour size of 3-5 cm can be treated with RFA)
- Patient with diagnosis of hepatic metastases particularly Neuroendocrine tumor.
- Bilirubin concentration less the 3mg/dl.
- Evaluation of patient by team specialist (Interventional Radiologist, cancer & Gastroenterology).
Pre Procedure: –
- Tissue Diagnosis
- Cross-sectional imaging of the liver ie Contrast-enhanced CT/ MRI confirming malignant nature.
- Laboratory studies including CBS, PT, PTT, Creatinine, liver function test and tumor markers.
Post Procedure: –
- 0-90% of patient suffers a post embolization syndrome characterized by pain, nausea and vomiting. These are controlled by medication.
- Vigorous hydration, IV antibiotics and antiemetic therapy.
- Neuroendocrine tumors may require chemoboembolization more than two times.
Contraindication: –
- Poor hepatic function
- serum bilirubin > 2-3 mg/dl
- no portal perfusion due to thrombosed main portal vein
Result in specific disease: –
Chemoembolization has become standard of care for un-resectable hepatoma and effectiveness in metastatic disease like.
- Colorectal metastases
- Ocular Melanoma
- Neuro-endocrine tumors
- Hepatoma
Advantages of chemoembolization
- Embolization, allows hepatic drug concentration to reach levels 10-25 fold higher than those achieved by simple intra-arterial infusion.
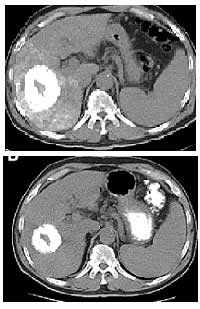
- Six month Follow-up case of Hepatic tumor: – Contrast enhanced CT scan shows significant reduction in size of liver tumor
- Chemoembolization also appears to increase the duration of therapy effect, with measurable drug levels being detected as long as a month post-infusion.
- Embolization of presinusoidal arterioportal shunts may facilitate selective drug delivery to the tumor, as the blood supply to normal liver is derived from the portal circulation while that supplying hepatic malignant cells almost exclusively from hepatic artery.
- Systemic toxicity is minimized even at high dose.
- Chemoembolization produces profound tumor ischemia at the time of drug administration, tumor hypoxia, is known to potentiate the effect of cytotoxic drug such as cancer medicine by inhibiting intracellular P-glycoprotein pump and increasing tumor cell uptake of drug.
Results: The results from various clinical study conducted in Medical University of Vienna, at Institut Gustave Rousy, Villejuif, France, at Barcelona Clinic Liver Cancer Group and a research study performed at John’s Hopkins Medical Institutions, Baltimore, Maryland shows: – complete response in 43% of patients, partial response observed in 28% of patients, objective response was 71% and complication in 4.3% of patients. (Depend up on the size of tumor and liver function).
Treatment with Multipolar RFA (Radiofrequency Ablation):-
RFA is an Interventional Non-surgical Treatment and is used in many conditions:
- Liver Cancer (HCC and metastasis)- for tumour size of 3-5 cm. For larger tumour, it may be combined with chemoembolization.
- Bone pain by Osteoid Osteoma
- Other cancers (kidney & lung)
- Varicose veins
Interventional Non-surgical Treatment
These procedures are performed without surgery by interventional radiologists. These physicians specialize in the use of X-rays, Digital subtraction angiography (DSA) and other techniques such as ultrasound, computed tomography (CT) and magnetic resonance (MR) to see inside the body without surgery. Flexible thin tubes (catheters) are inserted through skin or blood vessels and guided to the treatment (like heart angioplasty)
As it is done by interventional Radiologist, he can see inside the body without opening it through CT scan, ultrasound, DSA thereby treating exact site of disease without effecting surrounding structures. A video monitor & multipolar console displays real-time images of the lesion being treated.
RFA and Liver Cancer
Until recently, systemic treatment like chemotherapy was the only option for patients with inoperable liver cancer. Unfortunately, these medicines cannot be given in doses high enough to control most liver cancers because of their toxic effects, many of which are life-threatening.
RFA is a local treatment option for many cancers that cannot be surgically removed, and it does not have the unpleasant side effects of systemic options like chemotherapy. It is preferably performed on tumours of upto 5 cm size. For larger tumours, it can be combined with chemoembolization for better action of chemotherapy drug. Also
concomitant use of RFA helps in reducing the dosage of chemotherapy and thus reducing the side effects.
RFA in the Treatment of Other Cancers
In general, RFA is used for cancers that cannot be removed by surgeons because of their size or location, or because the patient is not healthy enough to have open surgery. RFA also is used to relieve pain and suffering for patients with a variety of cancers.
Kidney tumours – RFA alone is useful in tumours less than 4 cms in size. For larger tumor, it can be combined with embolization of tumor followed by RFA. Both of these are non-surgical treatment performed on one day hospitalization. Embolization helps in reducing the size while RFA kills the cancer cells.
Lung tumour – If tumour is producing intolerable symptoms, RFA helps to reduce the size of tumor, thereby reducing the symptoms.
RFA as a Treatment for Cancer Pain
Many patients have intolerable pain or other debilitating symptoms that can be relieved by RFA that shrink cancerous growth. The tumors themselves usually are not painful, but when they press against nerves, or interfere with vital organs, they can cause unbearable suffering. Within 1-4 wks of treatment with RFA, pain is relieved in majority of cases.
Role of RFA in CANCER THERAPY
RFA may be used alone, or in combination with other treatments, including surgery, chemotherapy and chemoembolization. Patients have remained disease free for several years after the treatment. Current strategies for using RFA include:
- Provide a local treatment option when surgery is not possible or too risky;
- Shrink large tumor to a size that makes it possible to remove them surgically;
- Relieve pain and other side effects to reduce suffering and improve the quality of life for people with cancer.
RFA in Osteoid Osteoma of bone
It is a local painful condition of bone, commonly seen in lower leg. Following detection by CT scan /MRI, RFA helps in complete pain relief by deactivating the cells without undergoing surgery.
RFA in Varicose Vein Treatment
RFA is the latest and most effective, patient-friendly and non-surgical treatment for varicose vein. Ablation of the vessel wall collapses the thick veins thereby directing the blood through normal veins. No bed rest, no side effects and no chances of recurrence. With the advent of RFA, surgery is no longer required as the mode of treatment for varicose veins.
Advantages of Interventional Non-surgical Treatment
- It is less risky as compared to surgery
- It is cheaper than traditional surgery.
- No surgical scar on skin.
- Procedure done under local anaesthesia.
- It is done as an outpatient (OPD) / day care or short hospital stay.
- Patients can resume normal activities within a day.
- It can fast relieve pain and suffering for many cancer patients
Its safety has been proven over many years in thousands of people
To explore best treatment options, call us at +91-98104-92778
Dr. Pradeep Muley is trained in the USA and Singapore and has performed over 20,000 non-surgical treatments for various diseases like uterine fibroids, uterine adenomyosis, un-operable liver tumor, liver abscesses, varicose vein, brain aneurysm and vomiting of blood from lungs and stomach. He runs the VARICOSE VEIN AND FIBROID CLINIC AT FORTIS HOSPITAL, VASANT KUNJ, NEW DELHI & created INDIA’S 1ST UTERINE FIBROID CLUB. He has treated the maximum number of fibroid patients in India through the innovative Uterine Artery Embolization method.
For more in-depth information on various non-surgical treatments available-
Mail Us: muleypradeep@hotmail.com or Visit to Website: – www.indianinterventionalradiology.com
Phone or Whatsapp: +91-9810492778